Journal : Quarterly Bulletin of the Clinical Society of the New York Post-Graduate Medical
School ; vol. i.
New York : Clinical Society, 1885-6.
Description : [1 l.] frontis., [1]-26 p. ; ill.: 4 phot., wood engravings, charts ; 24.5 cm.
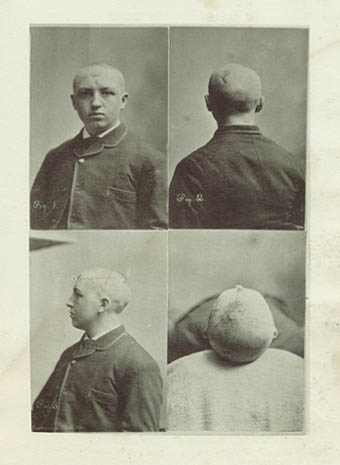
Photograph : four panel composite collotype—views of the subject's head.
Photographer : George Gardner Rockwood, 1832-1911.
Subject : Brain — Trauma surgery ; gun-shot wounds.
Notes :
The frontispiece is a photo-gravure made from photographs taken at the time. Photo. 1 shows the anterior scar; Photo. 2 shows the posterior scar; Photo. 3 is an absolute profile, and shows the path of the ball. The faint broad dark line marks the position of the fissure of Rolando; Photo. 4 shows the divergence of the path of the bullet from the median plane of the head.
The bullet entered at the centre of the forehead, an inch and a quarter above the upper level of the eyebrows; it passed in a straight line through the brain from a to b, and was deflected to c, where it lodged. Its place of lodgment was an inch and a half to the left of the posterior median line. The course of the ball is shown by the dotted line. The probe having been passed from a to b, that portion of the wound was eliminated in the further search for the bullet. The probe was then passed from b to c, after the same method as described for the exploration of a tortuous wound. The bullet could have been followed about three inches farther upon its deflected course till arrested by the tentorium, the end of the probe being exposed by a second counter-opening in the skull.—Page 21.
At the time he wrote this paper, Fluhrer was the Professor of Clinical Surgery at New York Post-Graduate Medical School and Hospital which was founded by William Hammond in 1882. Here, a candidate who successfully completed six months of courses and a final examination would receive a certificate of proficiency in neurology.
Fluhrer was also a visiting surgeon to both Bellevue and Mt. Sinai Hospitals. The subject of this tract, an operation for a self-inflicted gun-shot wound to the head, was conducted at Bellevue Hospital on January 24, 1884. By April 15 the patient had fully recovered, but was kept at the hospital, probably for observation. On May 22, Fluhrer exhibited his patient to his colleagues and the subject was judged to be in perfect health although Dr. Mittendorf found a limitation in the patient's visual field for the colors of green and red. Photographs were taken at this time, but the patient was not discharged until June 30th when he returned to his job as an assistant to a butcher.
The operation lasted 4 hours of which the first 2 1/2 hours were expended in an effort to stop a hemorrhage from a small artery just inside the superior convolution. Attempts to tie off the artery caused further laceration and it was necessary to leave a small artery clamp in place. The second part of the operation is a detailed description of the instruments and exploratory procedures taken to find the bullet and remove it from a trephine-hole behind the skull. Fluhrer debuts a tempered aluminum probe which can be bent to track the course of a bullet, but there is no indication that it is his invention. In this case the bullet was discovered to have rebounded from the inner wall of the pericranium and this position was marked with an "X" for trephining. During the May 22 lecture, Fluhrer speculated that had he found the bullet embedded near the center of the hemisphere, it was his intention to "push the ball on and to extract it through a posterior opening in the skull," and on page 23 he gives a lengthy description of such a procedure. In this case, however, the trephine-hole was enlarged with a rongeur forceps and the bullet was extracted from this point.
The most salient feature of Fluhrer's paper is his procedure for drainage, remarking from experience with previous cases of head injury, that "...good drainage had contributed to a favourable result, while, on the other hand, faulty drainage had sometimes led to disastrous consequences." Fluhrer describes two drains for this operation, the first one a small sized rubber tube which was tied with carbolized silk to the handle of a Nelaton probe and drawn through the wound, its ends trimmed and transfixed with safety pins. This drain was kept in place until January 31 when it was replaced by a second drain composed of two loops of catgut and 5 loops of horse hair which were left undisturbed for another week. On February 7, the catgut was found to be completely absorbed and 4 strands of the horse hair were removed. The following day Fluhrer detected evidence of "cerebral irritation" and decided to remove the remaining horse hairs. An accompanying chart graphs the patient's hourly temperature from February 7th to February 12 and shows a spike to 102° on February 9.
Knowledge of brain function is advanced by cases of head injury, but this subject revealed remarkably little behavioral changes other than a sporadic loss of short term memory. Soon after discharge from the hospital an accidental blow to the anterior scar from a sleeping companion caused severe head pain and an involuntary flexion of his limbs four hours later, first in his right limbs followed by his left limbs. He lost consciousness and was thrown from the bed by convulsions, but recovered sufficiently to go to work the following morning. A similar, but milder episode occurred on October 1st. Fluhrer found that a daily regimen of potassium bromide was essential.
In treating the hernić cerebri it was my aim to deal gently with them, at the same time keeping the wounds aseptic. In the period of their formation no pressure was made upon the brain protrusions. I looked upon their production as in part due to swelling of the cerebral tissue as a result of its injury, and based my non-interference upon the intolerance to pressure of acutely swollen or inflamed tissues. From this point of view, the openings, of considerable size, in the skull were a benefit in the treatment of the deep brain injury in its early stage rather than a disadvantage. In a later stage, however, when the brain protrusions had reached their greatest size and the course of the wounds had become chronic, I thought it advisable to aid the recession of the hernić by gentle and evenly applied pressure.—Page 20.
The photographs were taken by George Gardner Rockwood, who introduced the carte-de-visite format to America—the medium of his great success and fame in life. It is fun to speculate how his photographs of Dr. Fluhrer's patient might have inspired a medical hoax, "Brain pictures," that Rockwood wrote and published in the New York Tribune the following year (1887). His story made the claim that he participated in the autopsy of a mysterious german born philologist, Count Borenski. Using a microtome he purportedly acquired from the distinguished microscopist, Dr. John William Schmidt Arnold (1846–1888), Rockwood shaved off tissue samples from a bulge in the Broca region of the fictitious Borenski brain. From these shavings he prepared a sliver bromide photomicrograph that proved too grainy, but next he prepared an albumen plate of sufficient clarity to reveal a vermiform mass of legible characters from Ethiopic, ancient Syriac, and Phoenician languages.