Boston : Cupples & Hurd, 1888.
Description : [1]-167 p. ; ill.: 34 photo.s, fig.s, tab.s ; 25.5 cm.
Photographs : 34 photogravures of specimens to scale.
Subject : Prostate — Prostatectomy.
Notes :
Watson introduced perineal prostatectomy for the operative treatment of median enlargements of the prostate in 1889 (GM 4266). This atlas, because of its 34 full-scale photographic depictions of diseased specimens, served as the standard reference for radical surgery of the prostate, long after its text became outdated. More importantly, his work established the advantages of radical surgery over palliative procedures such as cannulation which were susceptible to infection and resulted in higher mortality rates. The following review appeared in The London Medical Recorder (London: Allen & Co., vol. ii., 1889; pages 211-212):
Operative Treatment of the Hypertrophied Prostate. By F. J. WATSON, M.D. Boston, U.S. 1888.
THIS handsome work contains the substance of an address delivered before the American Association of Genito-urinary Surgeons, at the fifth triennial meeting of the congress of American physicians and surgeons at Washington, Sept. 19, 1888, and is a valuable contribution to the surgery of the prostate. It is a very original work, and deserves to be carefully studied. The subject has been brought into special notice lately in England by the work of Sir Henry Thompson and Mr. Reginald Harrison, and by the observations of McGill, Mayo Robson, Whitehead, Buckstone Browne, and others, which we have already referred to in these pages. But we have in this work such admirable representations by the photogravure process of the specimens upon which the author's conclusions are based that we can judge with more facility than usual whether his conclusions are warranted. As many as thirty specimens of hypertrophied prostate are here depicted on quarto plates, and are excellent works of art, besides being very accurate representations of the originals. They are taken from specimens which the author has been able to meet with, and are new to English medical literature. Most of the plates contain a proportionately enlarged inch scale, which is a valuable addition, but the plates are said to represent the actual size of the specimens.
The objects sought in this work have been to lay down the lines which the author believes should govern surgical action in regard to the hypertrophied prostate ; to set forth the reasons which shall govern the choice of operation ; to demonstrate that operative treatment is surgically demanded in the appropriate cases — in the light of the evidence at our disposal and in contravention of the opposite opinions of Guyon, Thompson, Socin, and others ; to offer two adjuvants to the technique of the operation, the perineal drainage-tube and the galvano-cautery prostatectome ; and to contribute two clinical experiences.
He starts with the statement which we should be much inclined to question :—'Of all men beyond the age of 55 years we know that about one in every seven has an hypertrophied prostate,' and passes to the main subject of his inquiry, which is really the aggravated form of the disease. For these cases he is anxious to learn whether what he terms palliative or radical treatment is likely to be most serviceable. The palliative includes — I. Perineal drainage. 2. Suprapubic puncture with retained cannula. 3. Suprapubic cystotomy with retained cannula. The radical operations are — I. Division of the median enlargement by cutting instruments passed from the urethra — urethral prostatotomy. 2. Removal of the whole of the median enlargement by the same channel — urethral prostatectomy (Mercier and others). 3. The same operations done through an external perineal urethrotomy — perineal prostatotomy and prostatectomy. 4. Tunnelling the median enlargement through an external perineal urethrotomy (Harrison). 5. Suprapubic cystotomy and removal through this route of the median enlargement — suprapubic prostatectomy (McGill and others). 6. Division of the median enlargement by galvanocautery through the urethra from the meatus (Bottini). The methods of Heine, Newman, Biedert and others of iodine injection, cauterisation and electrolysis are not considered, as they have either failed or have not been attended hitherto with sufficiently reliable results. The author then gives briefly but clearly the technique of the various operations and the indications for the necessity of operation of some kind. But he finds no definite principles underlie the opinions formed by modern authorities on the choice of operation, and his object is to supply a rationale based upon an analytical study of the actual conditions encountered. And he gives a valuable series of cases which make the work of peculiar value to the surgeon and pathologist. Thirty cases are here depicted, but it is not clear to the reader from what sources they are obtained. However, as they are all full-sized photogravures of the original specimens they are likely to be of great use.
In studying these there are three points which he considers of special importance with reference to the choice of operation — I. The distance from the juncture of the membranous and prostatic urethras to the most distant point of the median enlargement within the bladder�the perineal distance. If this is not above three inches, the median enlargement can be reached by the finger through a perineal opening and effectually operated on from this part 2. The form of the median enlargement. If this be pedunculated or very salient, even if within reach from the perineum, the suprapubic operation will generally be preferable. Mercier's and Bottini's operations are only suitable when we know beforehand that we have to deal with a form approaching that of a bar at the neck of the bladder. 3. The small capacity and non-distensibility of the bladder or the reverse condition is another important matter to be considered. Bearing these three factors in mind, the author carefully examines his anatomical specimens with the following important results — that, contrary to the statement of Professor Guyon, the large majority of specimens do present such forms as to render radical operations possible and often easy — that in twenty-seven of the thirty cases the median enlargement formed the chief obstacle to urination — that in twenty-one of the thirty cases the median enlargement would have been successfully reached, incised or removed through the perineal route by any one possessing an index finger with a working length of three inches — that in ten, or nearly one-third of all the cases, the bladder was so small and incapable of distension as to render the suprapubic operation impossible. But we are not ourselves convinced on this last point, as the distensibility of the bladder cannot be shown by plates or even by preserved specimens. Continuing the summary, it is shown that in seven cases the great distance of the median enlargement from the perineum makes the suprapubic the only feasible operation. It is evident, therefore, that the anatomical forms and conditions are such that no one method is adequate for, or applicable to, all the varieties liable to be encountered. But we are more or less compelled to one or another according to the conditions met with.
Turning to the clinical evidences of the various operations he would inquire as to their total mortality, their relative mortality, and the permanency of their results, but he finds the records meagre, and gives tables of all the cases he can collect. He also adds two cases of his own — one of suprapubic prostatectomy in a very old man who died, and the other a case of perineal prostatotomy in a man of 74, who recovered.
The results arrived at in this work are that operative interference is not only justified but demanded in such cases, and it only remains to determine whether the palliative or the radical treatment is required. If the patient's condition is one of such exhaustion as to make a radical operation almost necessarily fatal, a palliative operation should be done, and for this the best is drainage through the perineum. Radical operations are, however, not more dangerous, and if successful accomplish much more. Mercier's and Bottini's operations from the meatus are applicable to only a limited number of cases. These are when a bar exists at the neck of the bladder, and are not easy to diagnose ; moreover, free drainage is difficult to secure. Of the cases described anatomically, two-thirds were operable through the perineum ; and, clinically, the perineal operation is safer than the suprapubic. The conclusion to be drawn is this :— In a given case open the membranous urethra, put in your finger and explore. Twice out of three times the operation can be completed by this route ; in the other third, the long perineal distance, or the form of the enlargement, will make the suprapubic operation necessary. When this is the case, and if at the same time the bladder can be distended so as to allow of the operation being done with the modern technique, proceed to do it at once or later. The author might have added that the preliminary perineal opening serves for subsequent efficient drainage.
Such is essentially an outline of this valuable work, and the author is to be congratulated upon his success in treating this important subject. It is a marked advance that he has made in trying to lay down some general principles which should guide us in selecting particular operations for the treatment of these cases, and it will be possible for a surgeon to see in these excellent photogravures arguments for or against special methods. Mention is just made of the tunnelling process of Mr. Reginald Harrison, and it is possible that surgeons will see that many of the specimens point to the advantage of such an operation ; but we cannot but recognise that the author has discussed the whole subject philosophically and without prejudice. We have pointed out that the evidence as to distensibility of the bladder in many cases is not conclusive, and would suggest that in some of the plates the position of the bladder when it has been cut away might be indicated by dotted lines so as to render the anatomical topography clearer. In one of the cases, or more, there existed very thin-walled pouches projecting from the bladder, and it is a possibility that distension of that viscus by injection might have proved fatal. — W. W. Flagstaffe.
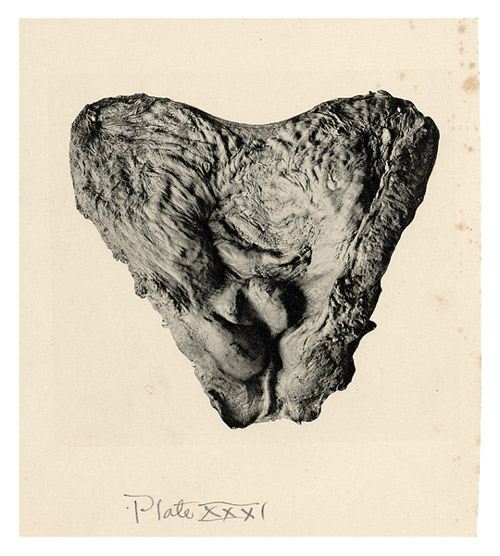
The following illustration was cut out of the book by the previous owner, Herbert Leslie Burrell, possibly intending to use it in a surgical compendium he was working on, but never finished. The plate number and caption are replaced by his handwritten inscription.
Perineal distance == 2 inches.
An irregular median enlargement and slight enlargement of the right lateral lobe. Coincident a thick-walled, not distensible bladder. The perineal operation is that of choice in this case.